

This attractive young lady appeared at my office with severe pain. Her upper right central incisor was very sensitive to percussion. The radiograph showed no obvious peri-apical pathology but there was an indication of some internal resorption. Endodontic therapy was initiated and on a subsequent visit completed. The tooth was restored with a composite restoration.

The upper right central incisor was very painful.

Note the marginal leakage on the mesial lingual composite restoration.

Upon entering the pulp chamber suppuration is evident and drainage is established.

Rotary burs are utilized for gross enlargement and cleaning of the canal prior to determination of a working length.
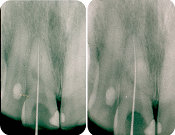
Working length was established with an electric apex locater and verfied with radiographs.

Access to the root canal should be large enough to thoroughly clean the entire pulp chamber and canal.

Following completion of the endodontics the patient presents for a composite restoration. Removal of the defective mesial composite causes bleeding which must be controlled prior to the placement of the composite.

Topical anesthesia is placed prior to the administration of xylocaine.

Xylocaine with epinephrine is utilized for hemostasis.

Gingival retraction cord is placed to help isolate the tooth.

An interproximal polishing strip is utilized to smooth the adjacent composite restoration.

Once the composite material is placed ( shade A-2 ) the occlusion is checked. This patient has an open bite so we are not concerned with trauma on this restoration.
Polishing protocol is followed.



Concerning the final aesthetic result, her appearance can be greatly enhanced via the utilization of crowns. I would hesitate to utilize more conservative porcelain veneers due to what appears to be abrasion and flattenning of her incisal edges due to a grinding habit. Veneers could fracture.