

The decision to perform third molar extractions should be based on the experience and know how of the dentist. Oral surgeons do this routinely. General dentists on the other hand may decide not to perform these procedures due to a number of factors.
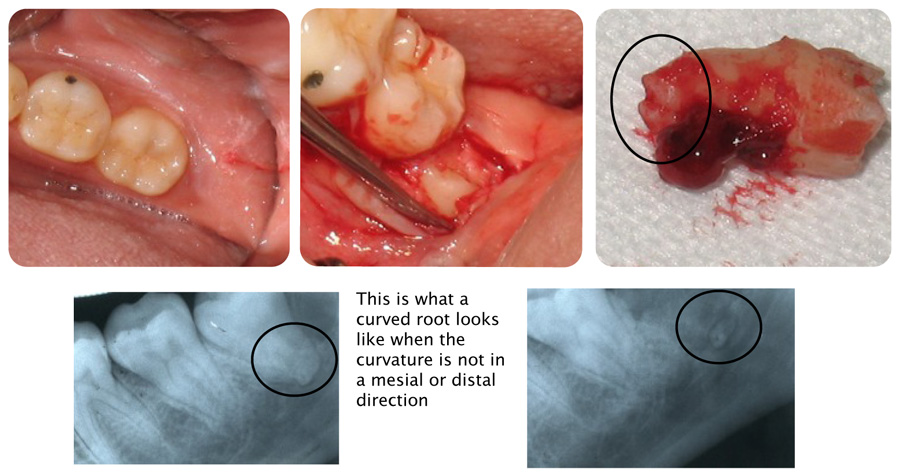
In this particular case I noticed a curved apical area on this third molar. This may create problems. The following therapy was performed. Local anesthesia was administered (topical plus carbocaine 3 % via a mandibular block). Septocaine was also administered via infiltration in the third molar mucosa. An incision was made and the mucosa was elevated revealing the third molar. The surrounding bone was resected in order to elevate this tooth out. Though the tooth became mobile initially I believe the apical curved root structure was preventing the extraction. Following removal of slightly more bone, the tooth was elevated out. Careful inspection of the tooth did reveal a small fracture of the apical root. This was verified on the post op radiograph. The patient was informed. Due to the proximity of this small root segment to the mandibular canal it was decided to leave it as is. I did give the patient 1000 mg. of amoxicillin (antibiotic) and a week’s supply of this medicine (20 tablets, 500 mg.). She was also given Vicodin ES narcotic analgesics and an ice pack. Written post operative directions were reviewed.
It is important to carefully think before trying to extract a root tip which is adjacent to a nerve. Before this patient left my office I called an oral surgeon friend of mine and discussed the situation with him. He agreed that I did the right thing by not trying to extract this root tip.
Post operative patient contact and evaluation
I always contact my patients the night after surgery to see how they are feeling. When I called this patient she said she had already found it necessary to take three Vicodin ES narcotics.
A few days later, she called me back and said she was fine. Initially, the night after surgery she couldn’t open her mouth and she had a fever. This was interesting because I believe that when she first came into the office as an emergency patient with swelling and pain her resistance was already compromised by the fact that she had contracted a bad cold. The point being always analyze a patient’s systemic medical condition. It has a bearing on surgical outcomes and post operative results.