

This patient had what initially appeared as shallow occlusal grooves that we were going to treat with sealers. Local anesthesia was administered (topical plus septocaine… septocaine works really well on these lower posterior teeth. Prior to our using this anesthetic we would usually need to administer a mandibular block injection).
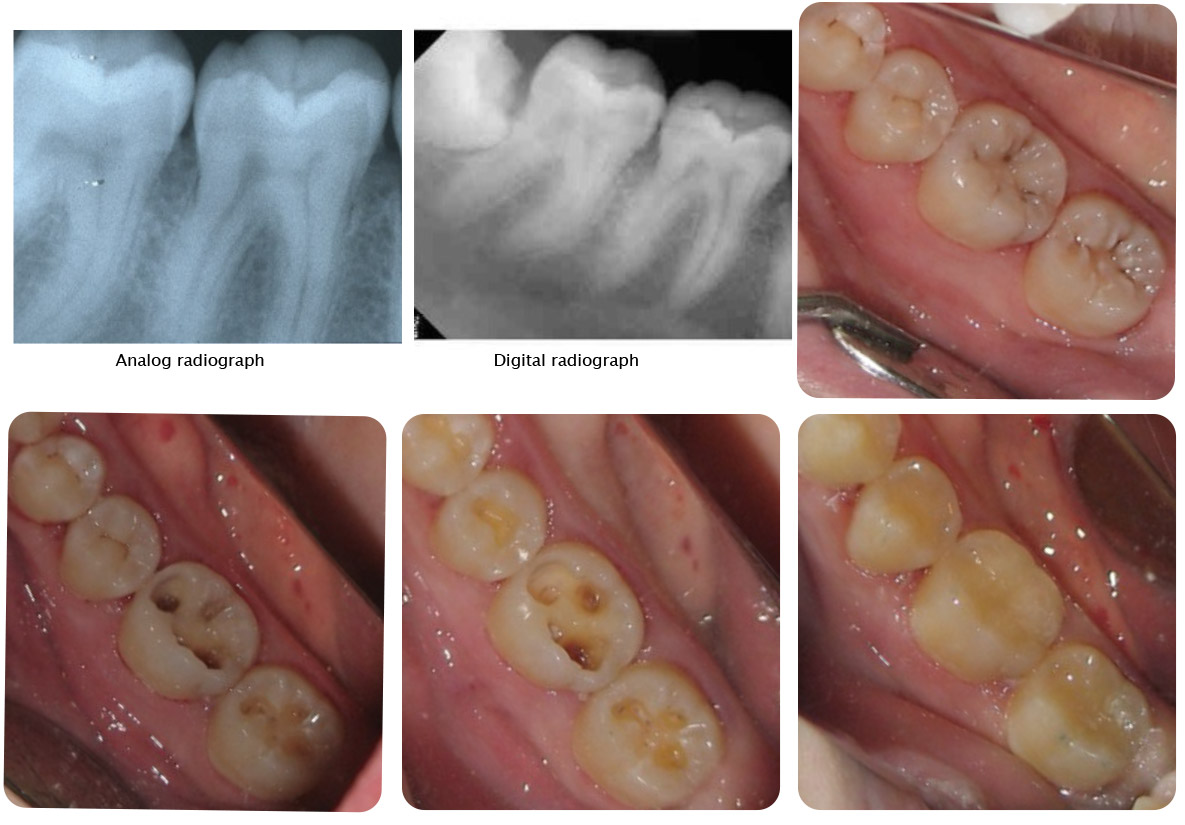
As we explored the lesions it became apparent that they were much deeper than we originally thought. This was not evident on our analog x-rays and when the patient had her recent digital radiographs sent here the lesions were not evident on these radiographs either. So the point is, be careful with what may appear to be shallow grooves and understand the limits of radiography. Of course resorting to better imaging such as cone beam tomography would be nice but is this overkill? Certainly when exploring these lesions and when using high powered magnification the decay becomes obvious.
Once all the decay was excavated floweable composite material were placed. Years ago we young dentists were taught to place a calcium hydroxide (dycal) base under deep restorations (this was called an indirect pulp cap as compared to when there is a nerve exposure and then it is referred to as a direct pulp cap). I have found that this is not necessary (we were also taught to place a cavity varnish under amalgam restorations). An endodontist neighbor of mine says that direct pulp caps don’t work and these exposed teeth eventually need root canal therapy… maybe… maybe not.