

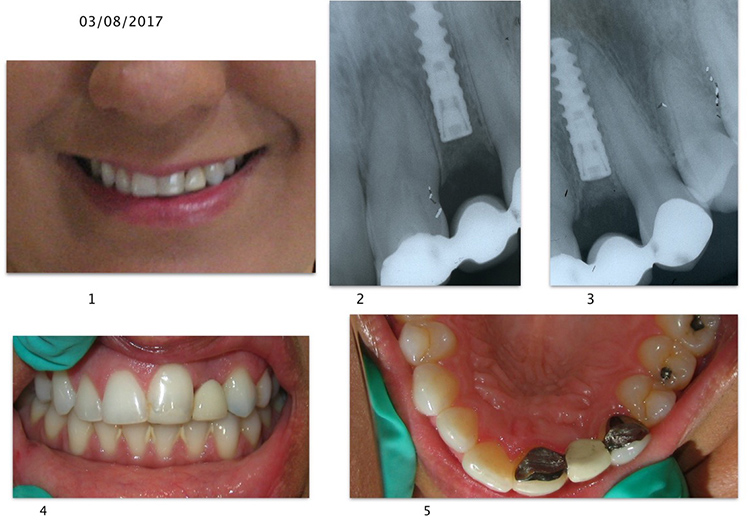
March 8, 2017. Initial appearance of patient with chief complaint of implant supported temporary crown and anterior aesthetics. A surgeon had placed this Nobel Active implant 3.5 x 13 mm. The implant is buried and a Maryland type bridge is in place.

 April 24, 2017. The area was anesthetized, the Maryland bridge was removed and access to the implant cover screw was achieved. The buccal flap was de-epithelialized and inverted to increase the degree of buccal soft tissue thickness.
April 24, 2017. The area was anesthetized, the Maryland bridge was removed and access to the implant cover screw was achieved. The buccal flap was de-epithelialized and inverted to increase the degree of buccal soft tissue thickness.
An implant level impression was taken and a stock temporary abutment was inserted (screw retained)
Due to the palatally placed implant fixture, prosthetic aesthetics was challenging.
 June 26, 2017. A transitional abutment /crown was fabricated. Note the degree of cantilever necessary to obtain an aesthetic result. This abutment was utilized as a means of creating a better emergence profile via application of composite material as necessary.
June 26, 2017. A transitional abutment /crown was fabricated. Note the degree of cantilever necessary to obtain an aesthetic result. This abutment was utilized as a means of creating a better emergence profile via application of composite material as necessary.
 After attempting to create a better emergence profile The tissue still appeared hemorrhagic though somewhat improved (this condition continued until the final restoration. When I consulted with Dr. Fred Witkin, a periodontist, he could not offer a definitive reason).
After attempting to create a better emergence profile The tissue still appeared hemorrhagic though somewhat improved (this condition continued until the final restoration. When I consulted with Dr. Fred Witkin, a periodontist, he could not offer a definitive reason).
 The overall final result shows definite improvements. We placed a full composite veneer on the upper left central incisor.
The overall final result shows definite improvements. We placed a full composite veneer on the upper left central incisor.
The upper left lateral incisor one piece abutment/crown was torqued down to 35 NC.
- labial concavity #10 (implant position)
- uneven gingival levels 8/9; reverse gull wing gingival architecture 8-9-11 (possibly extending to opposite canine ; #6). Tooth 11 is too short compared with planned restoration for #10. Gingival levels of 6-8-9-11 should all be even; while teeth 7 and 10 should be 2mm shorter. Her photos reveal a reverse gull wing gingival architecture.
- tooth # 9 requires full coverage due to extensive composite restoration
- Implant is positioned too far apically (approximately 7 plus mm apical to adjacent CEJ’s)
- unable to see pt’s smile line-some or all of these issues may or may not be a concern to her (?)
These issues were hopefully discussed with the patient pre operatively. If not, then she needs to be educated BEFORE the restorative procedure begins.
- Crn lengthening 8 and 6 and 11 to even gingival lengths
- Stage II implant #10 and place connective tissue graft
- 6-8 weeks of healing
- Crn #9, implant crn 10; Veneers 6-7-8-11( or full coverage as CEJ’s will likely be exposed)
Compromised plan:
- Crn Lengthen 8 to match 9
- Stage II / connective tissue graft 10
- healing period
- Implant crn 10; crn 9, veneer 8 (or full coverage as CEJ will likely be exposed)