

This 82 old female patient presented with generalized oral pain. She has been wearing an upper full denture for years. Her lower natural dentition was intact but showed signs of deterioration. She has been on multiple medications for years and due to the negative effect on salivary flow her clinical status is suffering.
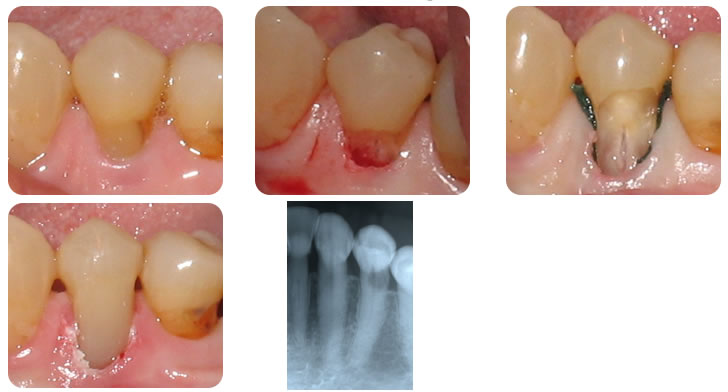
Following the taking of radiographs of her lower teeth, it was noticed that there was a radiolucency on the lower right first bicuspid. Clinically, there was no pathology and an intact cervical restoration.
The following therapy was performed today. Local anesthesia was administered (topical plus septocaine. Septocaine works great. In the past, prior to septocaine it would be necessary to administer a mandibular block injection). The composite was removed and the soft tooth structure apical this restoration was excavated out. There was no obvious decay. I t appeared that this lesion was some sort of root resorption. Though we were close to the nerve canal, there was no obvious exposure. The patient was advised though that endodontic therapy may be necessary in the future. The lesion extended about 2 mm below the gingival tissue. Considering that the patient had about 7 mm of attached gingival, I was able to resect some of her gingival tissue without encroaching on the less durable movable mucosa. If she would have had less attached gingiva to start I would have had to reflect and apically reposition this tissue. Gingival retraction cord was placed to isolate the lesion and xylocaine with 1 : 50, 000 epinephrine was administered to control the slight bleeding in the area. A flowable composite (shade A-4) was placed.